My scholarly project is an investigation of the possible sequelae occurring up to a decade after an osteomyelitis infection in a pediatric population. Acute hematogenous osteomyelitis (AHO) is an infection of the bone, seeded by a blood-borne organism. Annual incidence of AHO in the pediatric population of developed countries is approximately 1/5000-7700. Staphylococcus aureus accounts for up to 70-90% of AHO in otherwise healthy pediatric patients [1]. The increasing prevalence of community-acquired methicillin-resistant S. aureus (CA-MRSA) over the last two decades has resulted in the rise of such invasive pediatric infections in the United States [1-2].
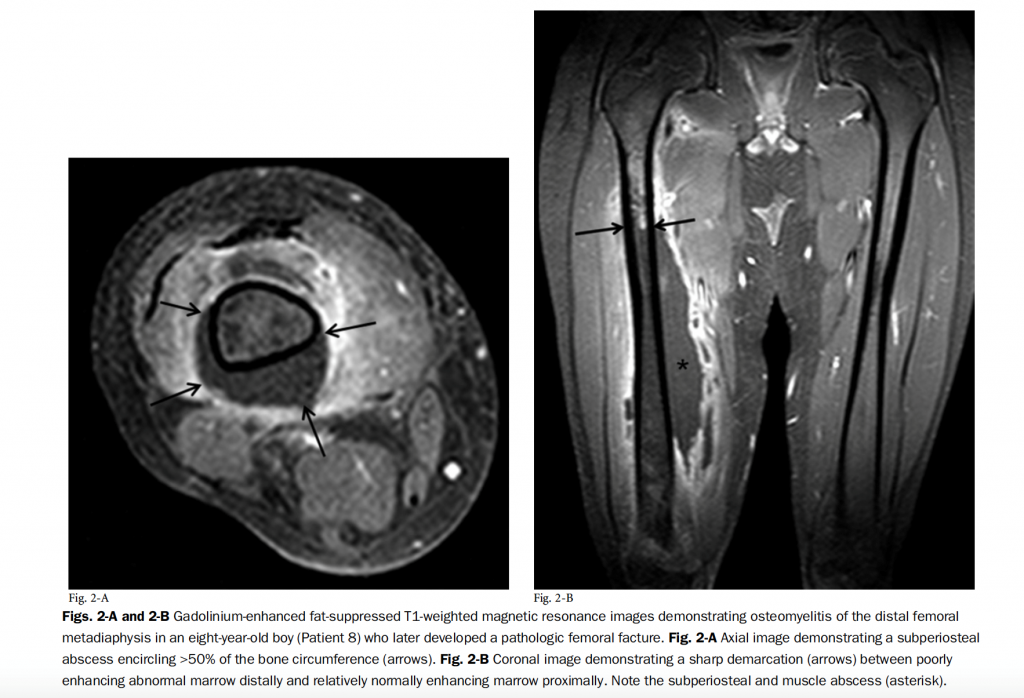
Pictures courtesy of Belthur MV, Birchansky SB, Verdugo AA, et al. Pathologic fractures in children with acute Staphylococcus aureus osteomyelitis. The Journal of Bone and Joint Surgery. 2012;94(1):34-42.
S. aureus is a gram-positive coccal bacterium in clusters that is catalase- and coagulase-positive. There are two main strains of S. aureus based on antibiotic sensitivities, methicillin-sensitive S. aureus (MSSA) and methicillin-resistant S. aureus (MRSA). MRSA contains the mecA gene that encodes for a low-affinity penicillin-binding protein in the bacterial cell wall that accounts for the organism’s ability to resist methicillin and other beta-lactam antibiotics [2]. Several virulence factors make S. aureus a more resistant and aggressive pathogen. One includes the ability to produce protein A, which binds the Fc portion of IgG antibodies, thereby inhibiting complement activation and phagocytosis. S. aureus also has the potential to produce toxic shock syndrome toxin (TSST-1), which is a superantigen that can lead to widespread, unregulated immunologic activation.
Arguably, the most important virulence factor in osteomyelitis is the Panton-Valentine leukocidin (pvl). Pvl is a cytotoxin that lyses white blood cells via pore formation and promotes tissue necrosis [3-4]. Pvl+ S. aureus AHO is associated with a more severe disease course than pvl– S. aureus [4]. The pvl gene can be found in both MRSA and MSSA but is seen much more commonly in MRSA, with studies citing up to 90% of pvl-containing S. aureus being MRSA [5]. This is a likely reason why CA-MRSA osteomyelitis tends to be more severe and results in a greater number of complications [1,5]. Pvl-positive S. aureus has not only been associated with a worse initial infection but also a greater number of sequelae in the first one to two years after the index infection. Examples of possible complications include pathologic fracture, growth plate arrest, chronic osteomyelitis, limb-length discrepancy, avascular necrosis of the bone, and deep venous thrombosis.
AHO with CA-MRSA as an etiology is still a relatively new phenomenon, having arisen around the turn of the 20th century. There are numerous studies that evaluate in-hospital and short-term outcomes of the disease course. However, with its relatively brief history, there is a gap in the literature regarding outcomes beyond one to two years of follow-up.
This is the gap that our study addresses. My scholarly project will investigate if and how these infections might affect a child’s function, development, activities of daily living, and likelihood of further complications as well as the extended prognosis of pediatric patients with these types of infections. My scholarly project mentor and the principal investigator of the study is Dr. Mohan V. Belthur, a pediatric orthopedic surgeon at Phoenix Children’s Hospital. Through a retrospective chart review and questionnaires sent to patients and their families, we will examine and compare differences in the outcomes of pediatric patients with an AHO infection caused by CA-MRSA vs. CA-MSSA more than 1 year following their index infection. Outcomes measured and compared will include complications, re-hospitalization, recurrence of infection, Pediatric Outcomes Documentation Instrument scores, and Activity Scale for Kids scores. The goal is to better understand the impact and likely outcomes of these types of infections, with the hope to ultimately improve treatment, care, and outcomes.
I would like to extend my sincere gratitude to both my Scholarly Project Mentor, Dr. Mohan Belthur, and Dr. Eric vanSonnenberg for their mentorship, guidance, time and effort spent in helping me develop and revise this article for The Differential. Thank you!
[2] Pendleton A, Kocher MS. Methicillin-resistant staphylococcus aureus bone and joint infections in children. Journal of the American Academy of Orthopaedic Surgeons. 2014;23(1):29-37
[3] Boyle-Vavra S, Daum RS. Community-acquired methicillin-resistant Staphylococcus aureus: the role of panton–valentine leukocidin. Lab Invest. 2007;87(1):3-9
[4] Crémieux A, Dumitrescu O, Lina G, et al. Panton–valentine leukocidin enhances the severity of community-associated methicillin-resistant Staphylococcus aureus rabbit osteomyelitis. PLoS ONE. 2009;4(9):e7204
[5] Gafur OA, Copley LAB, Hollmig S, Browne RH, Thornton LA, Crawford SE. The impact of the current epidemiology of pediatric musculoskeletal infection on evaluation and treatment guidelines. Journal of Pediatric Orthopaedics. 2008;28(7):777-785
 Tiana Blank is an Arizona native and a proud member of the class of 2018 at The University of Arizona College of Medicine – Phoenix. She attended University of Colorado at Boulder earning degrees in integrative physiology and psychology & neuroscience. Since the start of her medical school career, she has been involved in medical student government both as vice chair and class representative. Personal interests include spending time with family and friends, travel, running, laughter, and mind-body health.
Tiana Blank is an Arizona native and a proud member of the class of 2018 at The University of Arizona College of Medicine – Phoenix. She attended University of Colorado at Boulder earning degrees in integrative physiology and psychology & neuroscience. Since the start of her medical school career, she has been involved in medical student government both as vice chair and class representative. Personal interests include spending time with family and friends, travel, running, laughter, and mind-body health. Dr. Mohan Belthur is a full-time pediatric orthopedic surgeon at Phoenix Children’s Hospital. He is passionate about providing hope, healing, and high-quality family-centered healthcare to children and young adults with musculoskeletal problems to improve their quality of life. He also enjoys contributing to the training and education of residents and fellows. His current research interests include neuromuscular disorders, pediatric limb reconstruction, clubfoot, pediatric spine deformity, and musculoskeletal infection. In his spare time, he works with non-profit organizations to reduce the burden of childhood musculoskeletal disorders in developing countries.
Dr. Mohan Belthur is a full-time pediatric orthopedic surgeon at Phoenix Children’s Hospital. He is passionate about providing hope, healing, and high-quality family-centered healthcare to children and young adults with musculoskeletal problems to improve their quality of life. He also enjoys contributing to the training and education of residents and fellows. His current research interests include neuromuscular disorders, pediatric limb reconstruction, clubfoot, pediatric spine deformity, and musculoskeletal infection. In his spare time, he works with non-profit organizations to reduce the burden of childhood musculoskeletal disorders in developing countries.The Differential is a platform for UA COM-P medical students that aims to educate, inform and enlighten our community through collaborative dialogue and communication.